
BK and JC are two polyoma viruses that are not associated with symptomatic infection in immunocompetent individuals, but are commonly acquired and lie dormant. They may cause significant disease in immunosuppressed patients. JC virus has only very rarely been reported to cause renal disease, and the brain disease that it can cause is extremely rare in renal patients. Kidney infection by BK virus is a well recognised problem though. Published evidence of BK nephropathy is almost completely limited to renal transplantation.
BK virus (BKV) infects more than 80% of individuals by early childhood, and persists in epithelium of kidney, ureters and bladder. Viruria is common following renal transplantation, and testing for this is not helpful. Viraemia is less common, and sometimes (not always) associated with nephritis.
BKV associated nephropathy (BKVAN) is a tubulointerstitial nephritis that has often been mistaken for rejection, and carries a high risk of graft failure. There generally are no extra-renal symptoms or signs to suggest viral infection. The risk of BKVAN is highest in the first year after transplant. Occasionally it occurs later.
Screening and diagnosis
BKVAN is almost always associated with significant viraemia, making screening by PCR of blood potentially useful. Our protocol is to screen:
- First year after renal transplantation: Monthly for 6 months, at 1, 2, 3, 4, 5, and 6 months, then 3 monthly, at 9 and 12 months. 90% of cases have occured by 7 months in our cohort.
- Thereafter, six monthly testing at 18, 24 and 30 months – then stop, so a total of 2.5 years of surveillance.
- Indication testing could obviously occur after this routine surveillance period.
- The laboratory will not process a request if <4 weeks has elapsed since the previous result (unless that sample had a positive result).
- In the event of a first positive result, a follow up test in <4 weeks (but not < than 2 weeks) is warranted. In this instance, it should be specified on the clinical information that this is a follow up of a positive result to ensure the request is processed.
Diagnosis of BKVAN requires a renal biopsy, but the diagnosis may often be presumed if graft dysfunction is present in the context of a significant viral load. We increasingly do not biopsy to confirm BKVAN as the treatment is generally similar for BK viraemia and BKVAN and thorough screening means we generally detect BK infection in the early stages of it’s trajectory.
Management: reduction of immunosuppression
Reduction in immunosuppression is the cornerstone of BKV management. However there is no clear consensus on the viral load above which therapy should be altered but above 1,000 iu / ml (approximatley 10,000 copies / ml) appears to corrleate well with BKVAN.
The most robust data supports initially reducing or stoppping the antimetabolite (generally MMF), with later reductions in tacrolimus if viraemia or nephropathy persists. Other options include switching tacrolimus for cyclosporine or even sirolimus.
- Corticosteroids are generally continued at the same dose, as other agents are reduced
- Renal function and BKV levels should be monitored 2-4 weekly
- Check Donor Specific Antibodies (DSA) if the anti-metabolite is stopped for more than 4 weeks
After viral clearance – many practitioners see BK viraemia as a sign of over-immunosuppression and do not routinely return to previous dose of anti-metabolite. It may be necessary to balance this with perceived immunological risk, monitoring viral load.
This protocol has been used in Edinburgh, though use of alternative therapies is now rare (see below):
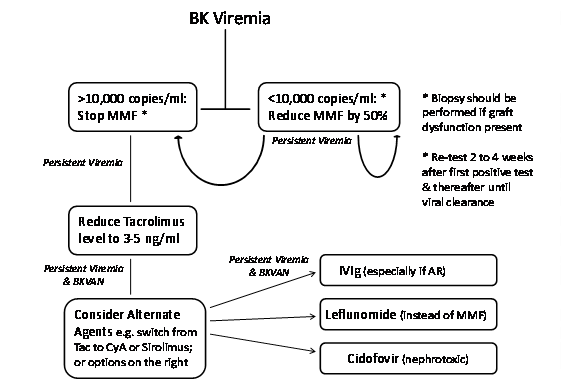
Alternative agents for BKVAN
These are all unproven and generally not indicated.
- IVIG – contain anti-BKV neutralising antibodies, but there is no robust evidence that it alters the course of nephritis.
- Leflunomide – has both immunosuppressive and antiviral activity. The therapeutic dose is uncertain and liver and bone marrow toxicity may occur. There are other significant side effects. There is no good evidence from clinical studies to support its use.
- Cidofovir – has modest in vitro antiviral activity agains BKV, but is itself nephrotoxic. Currently there is only very weak justification for using it or related compounds.
Concomitant BKVAN and acute rejection
This is a difficult diagnosis to be convinced about, as histologically TCMR and BKVAN can look very similar, unless vascular or microcirulatory injuries are present. The treatment is unclear and should be directed against the predominant lesion if that can be determined. Current viral load (and viral load trajectory) and DSA may help support the decision. IVIg may have a role.
Retransplantation
Retransplantation after graft loss from BKVAN has generally been successful, in the context of viraemia that has resolved.
Further info
- Info for patients about BKV (Edren)
Paul Phelan
Screening frequency updated at June 5th 2025 protocol meeting – PP