
CKD monitoring
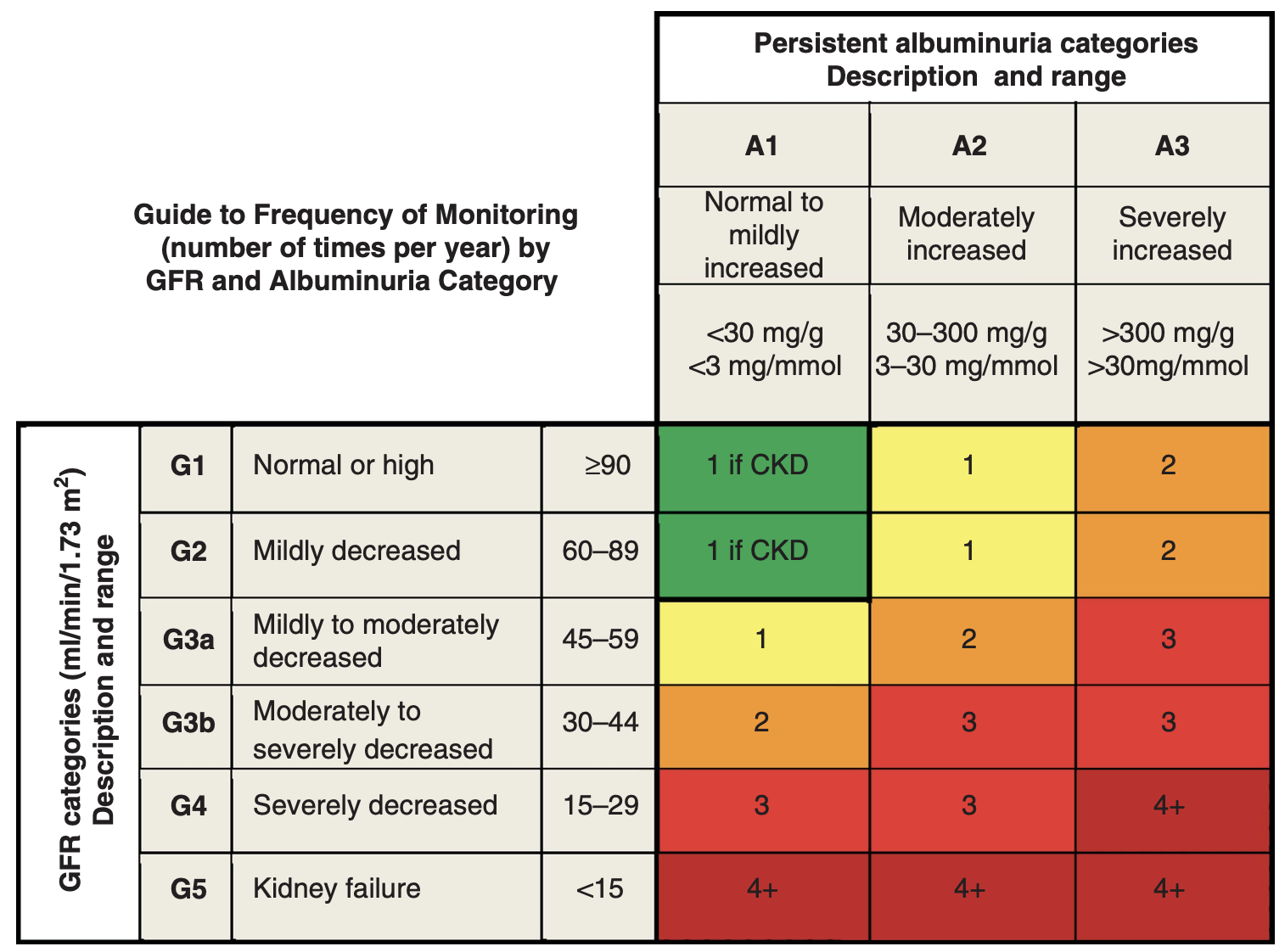
NICE and KDIGO (international consensus guidelines in kidney disease) have recommended that the frequency of CKD monitoring is stratified according to GFR and uACR (urine albumin:creatinine ratio) as in the figure below. The numbers (1 – 4+) are the number of recommended blood tests per year. This is a reasonable starting point, but common sense and principles of realistic medicine should be applied. For example, in frail multi-morbid patients, it may be appropriate to perform no routine monitoring at all.
NHS Lothian ICE CKD ordersets
The ICE ordersets used in primary care in NHS Lothian for CKD monitoring are:
- eGFR > 30: C&Es
- eGFR < 30: C&Es, alb, Ca2+, PO43-, FBC, urine albumin:creatinine ratio (uACR)
The ICE ordersets for CKD diagnosis are:
- eGFR > 30: C&Es, total cholesterol, HDL-C, urine albumin:creatinine ratio (uACR)
eGFR < 30: C&Es, total cholesterol, HDL-C, alb, Ca2+, PO43-, FBC, urine albumin:creatinine ratio (uACR)
The rationale for checking lipids at time of diagnosis is that CKD is an indication for considering lipid-lowering therapy, and if these are started then a baseline lipid profile may be helpful (e.g. if targeting a 40% reduction in non-HDL cholesterol as per NICE).
More selected testing
For many patients with CKD, if the likely cause is obvious (e.g. in context of longstanding hypertension / T2DM) then no diagnostic work-up is required.
The following scenarios suggest where additional testing may be helpful:
- suspected intrinsic kidney disease (e.g. if there are features of a multisystem disease): urine dip looking for blood and protein, spot urine sample for uACR (or uPCR), FBC, LFTs, Ca2+ and discuss with renal (who may suggest autoantibodies, complement levels, viral serologies etc.); if there is a strong suspicion of an intrinsic renal disease then we will probably wish to review in the renal outpatient clinic and direct investigations from there
- suspicion of myeloma: Ca2+, serum protein electrophoresis and a light chain assay (either urine Bence-Jones protein or serum free light chains); checking for both uACR and uPCR can be helpful (as the finding of a high uPCR but normal uACR would suggest overflow light chain proteinuria)
- unexplained CKD: renal ultrasound scan (to look for kidney size / symmetry / obstruction / cysts…)
- urinary tract symptoms / suspicion of prostatic disease: renal ultrasound scan