
You are the FY1 on the orthopaedic ward. A 64-year-old lady was admitted to hospital for an elective right total hip replacement. The operation goes to plan with no complications. However, 4 hours after her return to the ward she still hasn’t passed any urine. You are bleeped by the nurses to come and assess her.
You go to see her and start to take a focussed history.
What questions would you like to ask her?
Write down your answers prior to checking with our suggestions
When did she last pass urine?
Does she have a catheter in – long term or for operation?
How much fluid has she drunk over last day?
When was she fasting from?
When did she stop clear fluids?
How has she been recently – well vs. unwell?
Does she have any past medical history: diabetes, hypertension, systemic disease e.g. lupus?
Any family history of renal disease?
She thinks she last passed urine this morning before the surgery. She fasted from midnight and stopped clear fluids from 6am but thinks she had her last drink, a cup of tea, at about 9pm. She has not had any IV fluids. She has felt well recently. Her past medical history: T2DM, which is diet controlled and is well controlled. No relevant family history.
Another important question to ask is medication history.
Can you list any medications which may lead to renal impairment in the context of surgery?
– NSAIDS
– ACE -inhibitors, ARBs
– Diuretics
-Metformin and other hypoglycaemic medication
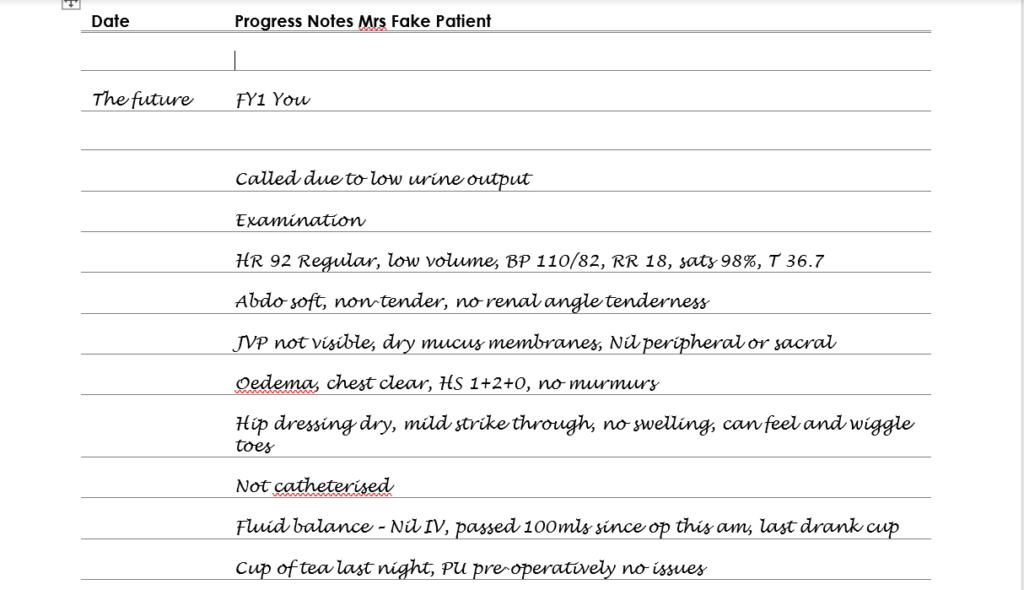
This lady has only been taking paracetamol as required for pain. You move on to examine her
What would you be looking for in your examination and what investigations would you like?
For each of these, try to write your own lists before revealing the answers
As with all patients – if your patient was unstable start an A-E assessment and escalate as appropriately.
As she is currently stable
- Check catheter – kinked, patent, draining, volume?
- Assess fluid status: mucous membranes, JVP, pulse (rate and volume), skin turgor, oedema – peripheral and sacral, hypotension is a late sign
- Fluid replacement – has she had any? What rate?
- Abdo / renal exam – any tenderness?
- Examination of any wounds, drains etc
Observations – repeat these currently and compare to those pre-operatively and intra-operatively – looking at intra-operative observations may indicate hypotension in the operation or the degree of change between them may indicate potential causes for presentation
Blood tests – repeat bloods if possible and compare values to pre-operative values. Especially U+Es (creatinine rise? , dehydration?) and full blood count (bleeding? , hypovolaemia?)
Further investigations will depend on what you find in your examination
Returning to your patient
You decide that you need to take some further action for Mrs Fake Patient
Select what you feel describes the best action
This is not the best option here and in fact may cause your patient to further deteriorate and become sicker.
Yes fluid is correct. There may be another answer that is pertinent.
Although we do not have haematology results back, there is no evidence of acute bleeding presently. Therefore this is not the most appropriate answer.
Correct. This is the only way we can determine whether any intervention is of any benefit in this situation and indeed any situation where a patient has deteriorated.
This is not required. Mrs Fake Patient can feel and wiggle her toes. If there was ongoing dense paresis then this could be considered
On a piece of paper prescribe the type of fluid and rate at which you would prescribe it, then select reveal when you have completed this.
500ml of any crystalloid as a bolus (rate 999mls/hr). Then reassess.
With this treatment her heart rate stabilises to 72bpm and BP comes up to 134/76. You determine that she is intravascularly deplete likely due to dehydration following prolonged fasting. You decide to prescribe some further background intravenous fluids and encourage Mrs Patient to drink.
You ask that a strict fluid balance be recorded and plan to review her later in the day.
You review her and prescribe a further bag of fluids. On further review later that day you see that she has passed 237ml of urine in 3hours.
Is this sufficient for this lady? How would you determine this?
Yes. Aim for 1ml/kg/hour. If we say the average woman is 60-70kg then that would be 60-70ml/hr (180 – 210ml over 3 hours).
Mrs Patient’s urine output returns to normal over 24 hours and the rest of her admission is uneventful. She completes her physio and is discharged without further complications. You determine her initial low output was due to dehydration and encourage her to increase her oral fluid intake.
Well done you have completed the case.
Further resources